So we are a little over half way in this series. We have been developing an understanding of the core components of a mental state exam so that we can support our young people as best we can. This week I was speaking with a youth worker in one of Victoria’s largest Christian denominations about a mental health conference he was at. I was reminded about how important it is for all youth workers to have a strong understanding of mental health. So far we have discussed how a young persons appearance, behaviour, speech and language, and their mood and affect can provide indicators as to their mental state. Today we discuss how a young persons thought content can provide insight into their current mental health status.
 |
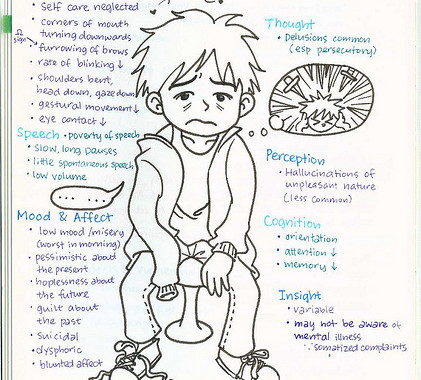
| A prime example of maladaptive thought content and process |
Thought process
A young person’s thought process can tell you a lot about them. The quantity, tempo and form of thought are keys to understanding the process. A persons thought process can’t be directly observed. It can only be described by or inferred from a young persons speech. Some people may experience their thoughts coming so rapid that their speech seems incoherent. Alternatively an individual may have inhibited thinking, in which thoughts seem to progress slowly with few associations. Are they all over the place or are they clear and consistent. do they have few thoughts or do they keep returning to the same thoughts.
Does the young person include a great deal of irrelevant detail or make frequent diversions, but remains focused on the broad topic. Flight of ideas is typical of mania. On the other hand, young people with depression may have slow or inhibited thinking. Poverty of thought is one of the symptoms of schizophrenia, and may also be a feature of severe depression.
Thought content
When we think of thought content we would describe a young persons delusions, overvalued ideas, obsessions, phobias or preoccupations. To draw out any abnormalities of thought content we need to explore a young persons thoughts in an open-ended conversational manner with regard to their intensity, salience, the emotions associated with the thoughts, the extent to which the thoughts are experienced as one’s own and under one’s control, and the degree of belief or conviction associated with the thoughts.
A delusion is a core feature of psychotic disorders. A young persons delusions may be described as persecutory or paranoid, delusions of reference, grandiose, erotomanic, delusional jealousy or delusional misidentification. Delusions may be mood-congruent (the delusional content is in keeping with the mood), or mood-incongruent (delusional content not in keeping with the mood). An overvalued idea is a false belief that is held with conviction but not with delusional intensity. Hypochondriasis is an overvalued idea that one is suffering from an illness and people with anorexia nervosa may have an overvalued idea of being overweight.
Preoccupations are thoughts which are not fixed, false or intrusive, but have an undue prominence in the person’s mind. Clinically significant preoccupations would include thoughts of suicide, homicidal thoughts, suspicious or fearful beliefs associated with certain personality disorders, depressive beliefs (for example that one is unloved or a failure), or some types of anxiety and depression. A Mental State Exam contributes to risk assessments of young people by including a thorough exploration of any suicidal or hostile thought content. Assessment of suicide risk includes detailed questioning about the nature of the person’s suicidal thoughts, belief about death, reasons for living, and whether the person has made any specific plans to end his or her life.
Stay tuned next week for part six: Perception
If you haven’t yet, sign up for our newsletter to find out all the goings on at Ultimate Youth Worker. (Sign up here)